“Social” was the original term for the non-medical indication to freeze eggs, but it carried a pejorative connotation, as if women were frivolously freezing eggs simply for convenience. (The hype of egg freezing parties at some clinics where people gathered to drink champagne and sign up for treatment also fueled critics). “Elective” became the preferred term and is still commonly used, indicating that the people are making a choice to freeze, even if not medically necessary. More recently “planned” egg freezing appears to be the latest label of choice. I like it: it implies an intentionality to the process, that a person is taking control of their fertility.
Where the advent of oral contraceptive pills in the 1960’s was revolutionary in allowing women to prevent pregnancy, egg freezing is an innovation that allows choice on the other end of the reproductive spectrum: it can help preserve the chance of biological motherhood which many in generations past had to compromise to pursue academic, career, and other opportunities. Like “the pill”, egg freezing has its limitations: it can’t help everyone. (On another note, not to get too political, but it is a shame that in a country that takes pride in protecting reproductive choice, there is no federal support for infertility or egg freezing in Canada. Given the associated expense, for those not employed by the companies that cover the costs, it is financially out of reach for many who could benefit the most. But I digress…)
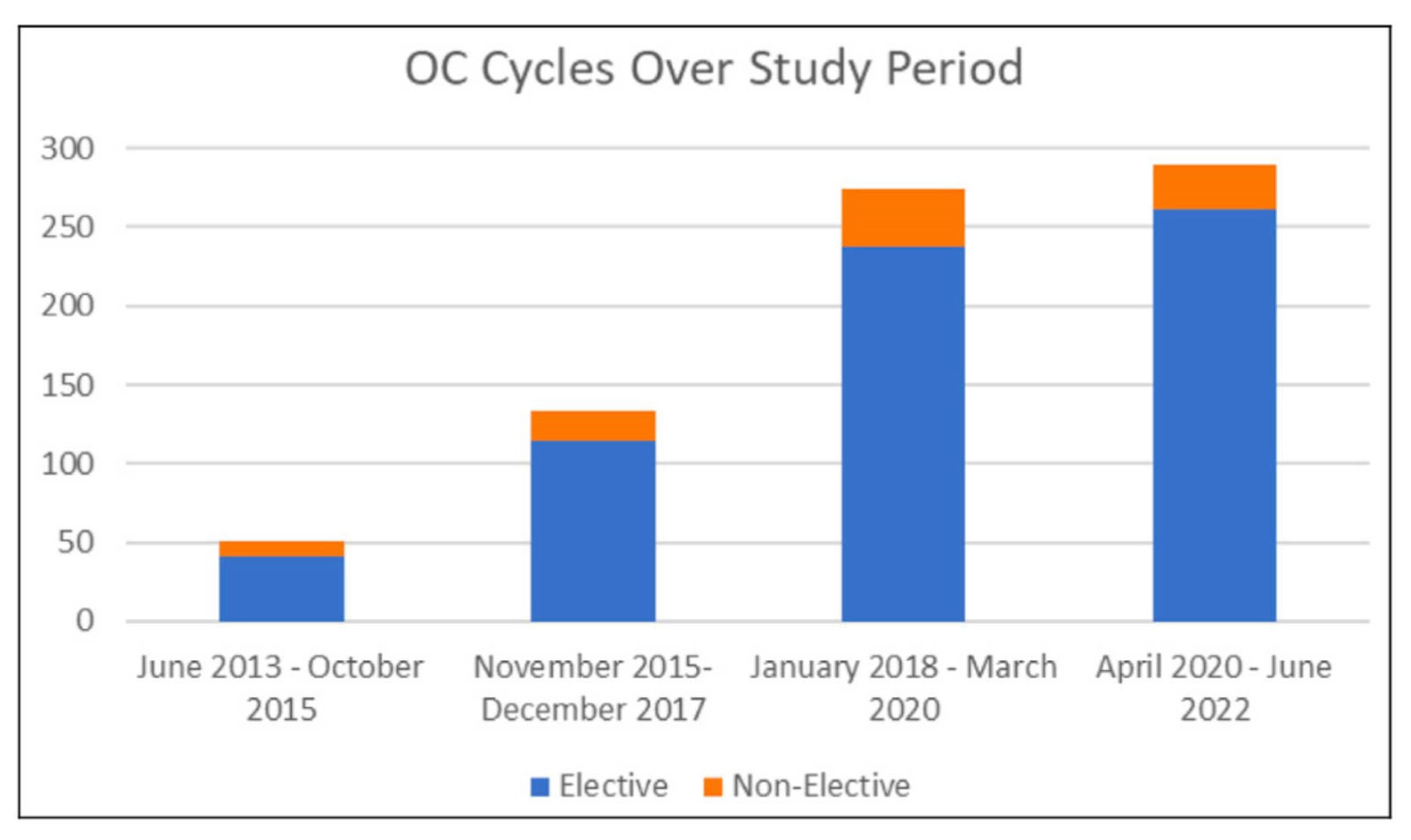
An interesting piece was just published in the New York Times that documents the experience of egg freezing through the stories of 7 women who went through the process. The personal stories are relatable. As one would anticipate, not all have happy endings. The article alludes to the fact that while the number of people who have frozen eggs has increased by 400% between 2012 & 2020 (in line with our data), there is still very little published data about the outcomes. Virtually every clinic will tell you that they can freeze eggs, but few can provide statistics about what happens when patients return to use them.
That, however, is not a dig on other clinics: the fact is that we don’t really have all the facts since most patients have not come back to use their eggs. In our series of 646 patients who had their oocytes vitrified, only 65 returned to fertilize. However, the patients who returned were older at the time of freezing, and many already had very low ovarian reserve with few eggs retrieved. Just like in the NYT article, not all outcomes were favourable in our series: there were 2 patients who did not have any eggs survive the thaw, and 5 who did not have normal fertilization. (Notably, 6 of these patients only had 1 egg each and the 7th had only 4 eggs; not exactly the ideal candidates for egg freezing.) There were several others whose embryos did not develop to the blastocyst stage, and others still who had their blastocysts tested with PGT-A but did not have any normal embryos. These are the same challenges that we face every day with routine IVF.
Happily, there were many positive outcomes from our cohort, too. In fact, 65% of patients who had an embryo transfer had a healthy delivery or ongoing pregnancy. Furthermore, 2 patients who both froze the eggs in their late 30’s had 2 babies each from their respective single egg freezing cycles (including the amazing Natalie, whose story you can read here). The oldest age at which eggs were frozen then thawed to successfully lead to a healthy pregnancy: 43 (and she returned when she was 49).
We reported our statistics openly and candidly, with the caveat that the experience of these 11% of egg freezing patients that have come back to use their eggs still doesn’t give us a clear picture of what the outcomes will be for everybody else. Not until many more women come back to use their eggs can we state with statistical confidence how well it really works.
While the data purist in me hesitates to speculate, I will do so anyway: egg freezing DOES work. The challenge is not so much the technology, as vitrification is refined to the point that the process is almost ready for full automation. However, if we don’t have healthy eggs to work with in the first place, we can’t expect much when we try to use them in the future.
“If I don’t freeze my eggs, can’t I just try later IVF if necessary?” Yes, of course IVF is an option if ovarian reserve and age are still reasonable. We help patients on a daily basis become parents into their 40’s with IVF. However, according to a recent study in Fertility & Sterility, for people interested in deferring childbearing, freezing eggs in the early 30’s is a more successful and cost-effective approach than resorting to IVF beyond 40.
So how to decide if you should freeze your eggs? Just talk to your Olive doctor. We don’t have a crystal ball yet, but we have evidenced-based calculators to predict how many eggs we can expect to retrieve based on your age and AMH level, and subsequently the estimated live birth rate. After your eggs are retrieved, we take a picture of each one to analyze with Violet, the AI-driven computer vision tool which generates a more personalized probability for outcome expectations.
And then you live your life… you may never have to use your frozen eggs. It is certainly quite possible (probable, really) that you will conceive naturally if/when you decide to start trying. However, the consistent feedback I get from my patients after egg freezing is that while they accept that there are no guarantees, knowing that they have done what they can to position themselves for future motherhood without derailing their personal goals provides peace of mind.