Remember that slacker in high school who barely got by with a C-average who is now more successful than the grade-A bookworms? Grades weren’t so important after all.
What about when it comes to embryo grading? Just like the report card is meant to reflect scholastic aptitude, grading in the IVF lab is meant to tell us something about embryo competence. However, in embryology as in school, grades aren’t everything.
First, let’s establish how we grade embryos. Specifically, we’re talking about blastocysts, the stage a viable embryo reaches 5-7 days after the egg is fertilized. The standard for blastocyst grading was devised by Dr. David Gardner, the prolific embryologist responsible for many contributions to the field of human embryology. A blastocyst is composed about 100-200 cells depending on its maturity, but it is not possible to accurately count the cells, so the grading is based on qualitative features that can be observed through the microscope.
The Gardner grading rubric consists of three parameters: a number followed by two letters; for example, 3BC, 5AA, etc. The number refers to the expansion of the blastocoele, which is the fluid filled cavity of the blastocyst. The first letter represents the inner cell mass (ICM), which are the cells from which we develop. The second letter represents the trophoectoderm (TE) which gives rise to the placenta. A combination of one choice from each column will define the blastocyst grade.
EXPANSION
1: Early blastocyst, with a cavity less than half the volume of the embryo.
2: A cavity filling more than half of the embryo.
3: Full blastocyst with cavity completely filling the embryo.
4: Expanded blastocyst, cavity larger than the embryo with a thinning shell (aka, “zona pellucida”).
5: Hatching blastocyst, part of the embryo is starting to hatch out of the shell.
6: Hatched blastocyst, the embryo has completely emerged from the zona pellucida.
INNER CELL MASS
A: Tightly packed, many cells.
B: Loosely grouped, several cells.
C: Few cells loosely grouped.
TROPHOECTODERM
A: Many cells forming a cohesive layer.
B: Few cells forming a loose layer.
C: Very few cells forming a sparse layer.
To complicate matters, many clinics including Olive, use a modified grading system which substitutes “CB” (cavitating blastocyst) and “EB” (early blastocyst) to differentiate development in stage 1.
The rationale for the Gardner grading system is based on the expectation that an embryo must dynamically change during early development. Dynamic is the key word here, because the expected milestones are separated in matters of hours. We can witness blastocysts change before our eyes (if our eyes are looking through a microscope, that is).
Embryos that don’t reach the blastocyst stage in the lab are clearly not viable. If an embryo has reached the blastocyst stage, the grading system is designed to select the most likely to implant.
Herein lies the rub: identifying bad embryos is easier than picking the good ones. In other words, if the embryo development arrests in the lab, we can say with confidence that it is clearly nonviable. Yet, if an embryo has reached the blastocyst stage, regardless of the grade, the best we can do is give it the benefit of the doubt.
If a patient has multiple blastocysts, grading gives us a methodical approach to prioritize embryo selection. Less developed blastocysts may signal an arresting trajectory, while higher grading suggests more promising development. However, like the tortoise and the hare, getting to the finish line is not all about speed.
Furthermore, grading tells us nothing about chromosomal abnormalities. We need PGT-A to do that: ask any patient who has had gone through PGT-A with many beautiful blastocysts only to find out that all were chromosomally abnormal (aneuploid). Without PGT-A, we can only hope that the blastocyst is chromosomally normal and give it a chance.
Finally, while our embryologists are highly trained and exceptionally skilled, grading based on the human assessment is prone to subjectivity. Give a picture of an embryo to an embryologist on Monday morning, then turn it upside down and given it back to them on Friday afternoon: it’s quite possible that the same embryo will receive a slightly different grade. Innovations in computer vision and AI promise to provide more consistency in grading but the benefits of these systems are still not completely proven.
So, if grading is not predictive of outcome, why do we bother? It is at least useful to rule out the obviously nonviable embryos and prevent futile transfers. It is also helpful to have a standardized (if imperfect) method to communicate about embryo quality. Grading also helps us maintain quality control in the lab which allows us to track our outcomes and refine techniques over time.
Bottom line: embryo grading is helpful but far from an exact science. Many low-grade blastocysts turn into beautiful babies. Speaking on behalf of late bloomers everywhere, sometimes they just need a chance.
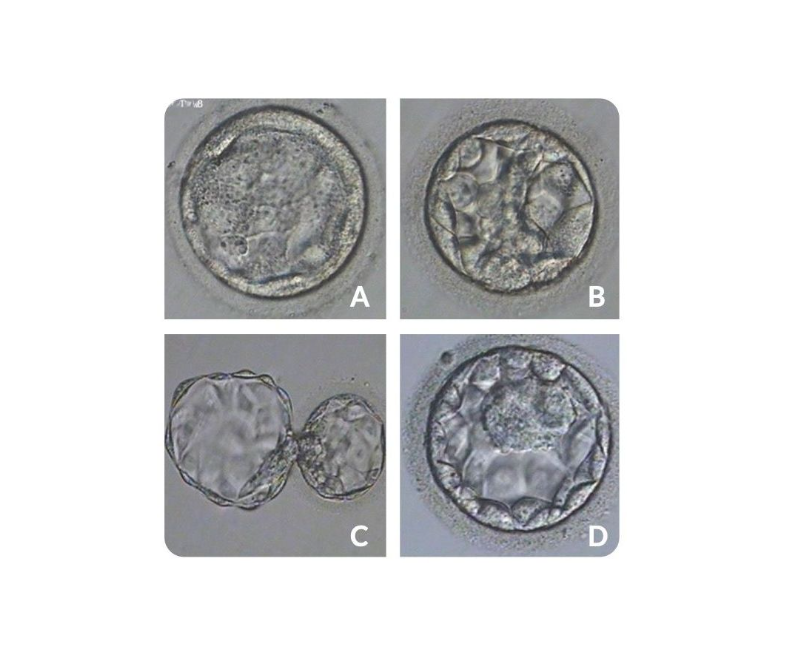
Speaking of grades, pop quiz!
1) Grade the following embryos, and 2) determine which one resulted in a healthy baby.